You are using a browser that is not supported by this site. The site will not function properly. Please switch to the latest version of a supported browser such as Chrome, Safari, Edge, or Firefox to use this site.
REMODULIN IS A PROSTACYCLIN-CLASS THERAPY1
PROSTACYCLIN IS IMPORTANT FOR NORMAL LUNG FUNCTION2
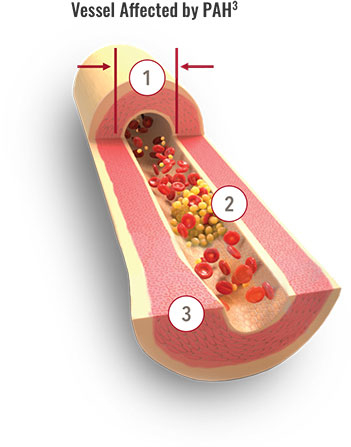
Treprostinil mechanism of action (MOA) targets 3 of the major pathologic changes that occur in PAH1,3,4
Vasoconstriction
Treprostinil directly dilates pulmonary and systemic arterial vascular beds
Platelet aggregation
Treprostinil inhibits platelet aggregation
Smooth muscle proliferation
Treprostinil inhibits smooth muscle cell proliferation
The Prostacyclin Pathway
Abnormally low levels of prostacyclin are linked to PAH disease severity and progression. Watch this video to learn more about how treatments like treprostinil aim to compensate for missing prostacyclin.
PAH=pulmonary arterial hypertension.
Remodulin® (treprostinil) Injection
Important Safety Information for Remodulin
Warnings and Precautions
- Chronic intravenous (IV) infusions of Remodulin delivered using an external infusion pump with an indwelling central venous catheter are associated with the risk of blood stream infections (BSIs) and sepsis, which may be fatal. Therefore, continuous subcutaneous (SC) infusion is the preferred mode of administration.
- Avoid abrupt withdrawal or sudden large reductions in dosage of Remodulin, which may result in worsening of PAH symptoms.
- Titrate slowly in patients with hepatic insufficiency, because such patients will likely be exposed to greater systemic concentrations relative to patients with normal hepatic function.
- Remodulin is a pulmonary and systemic vasodilator. In patients with low systemic arterial pressure, treatment with Remodulin may produce symptomatic hypotension.
- Remodulin inhibits platelet aggregation and increases the risk of bleeding.
Adverse Reactions
- In clinical studies of SC Remodulin infusion, the most common adverse events reported were infusion site pain and infusion site reaction (redness, swelling, and rash). These symptoms were sometimes severe and sometimes required treatment with narcotics or discontinuation of Remodulin. The IV infusion of Remodulin with an external infusion pump has been associated with a risk of blood stream infections, arm swelling, paresthesias, hematoma, and pain. Other common adverse events (≥3% more than placebo) seen with either SC or IV Remodulin were headache (27% vs. 23%), diarrhea (25% vs. 16%), nausea (22% vs. 18%), rash (14% vs. 11%), jaw pain (13% vs. 5%), vasodilatation (11% vs. 5%), edema (9% vs. 3%), and hypotension (4% vs. 2%).
Drug Interactions
- Remodulin dosage adjustment may be necessary if inhibitors or inducers of CYP2C8 are added or withdrawn.
Specific Populations
- In patients with mild or moderate hepatic insufficiency, decrease the initial dose of Remodulin to 0.625 ng/kg/min of ideal body weight, and monitor closely. Remodulin has not been studied in patients with severe hepatic insufficiency.
- Safety and effectiveness of Remodulin in pediatric patients have not been established.
- It is unknown if geriatric patients respond differently than younger patients. Caution should be used when selecting a dose for geriatric patients.
- There are no adequate and well-controlled studies with Remodulin in pregnant women. It is not known whether treprostinil is excreted in human milk or if it affects the breastfed infant or milk production.
Indication
Remodulin is a prostacyclin vasodilator indicated for the treatment of pulmonary arterial hypertension (PAH; WHO Group 1) to diminish symptoms associated with exercise. Studies establishing effectiveness included patients with NYHA Functional Class II-IV symptoms and etiologies of idiopathic or heritable PAH (58%), PAH associated with congenital systemic-to-pulmonary shunts (23%), or PAH associated with connective tissue diseases (19%).
In patients with PAH requiring transition from epoprostenol, Remodulin is indicated to diminish the rate of clinical deterioration. Consider the risks and benefits of each drug prior to transition.
REMISIhcpFEB2025
Please see accompanying Full Prescribing Information for Remodulin.
For additional information, visit www.RemodulinPro.com or call Customer Service at 1-844-UNITHER (1-844-864-8437).
For additional information, visit www.RemodulinPro.com or call Customer Service at 1-844-UNITHER (1-844-864-8437).
Remodulin® (treprostinil) Injection
Important Safety Information for Remodulin
Warnings and Precautions
- Chronic intravenous (IV) infusions of Remodulin delivered using an external infusion pump with an indwelling central venous catheter are associated with the risk of blood stream infections (BSIs) and sepsis, which may be fatal. Therefore, continuous subcutaneous (SC) infusion is the preferred mode of administration.
- Avoid abrupt withdrawal or sudden large reductions in dosage of Remodulin, which may result in worsening of PAH symptoms.
- Titrate slowly in patients with hepatic insufficiency, because such patients will likely be exposed to greater systemic concentrations relative to patients with normal hepatic function.
- Remodulin is a pulmonary and systemic vasodilator. In patients with low systemic arterial pressure, treatment with Remodulin may produce symptomatic hypotension.
- Remodulin inhibits platelet aggregation and increases the risk of bleeding.
Adverse Reactions
- In clinical studies of SC Remodulin infusion, the most common adverse events reported were infusion site pain and infusion site reaction (redness, swelling, and rash). These symptoms were sometimes severe and sometimes required treatment with narcotics or discontinuation of Remodulin. The IV infusion of Remodulin with an external infusion pump has been associated with a risk of blood stream infections, arm swelling, paresthesias, hematoma, and pain. Other common adverse events (≥3% more than placebo) seen with either SC or IV Remodulin were headache (27% vs. 23%), diarrhea (25% vs. 16%), nausea (22% vs. 18%), rash (14% vs. 11%), jaw pain (13% vs. 5%), vasodilatation (11% vs. 5%), edema (9% vs. 3%), and hypotension (4% vs. 2%).
Drug Interactions
- Remodulin dosage adjustment may be necessary if inhibitors or inducers of CYP2C8 are added or withdrawn.
Specific Populations
- In patients with mild or moderate hepatic insufficiency, decrease the initial dose of Remodulin to 0.625 ng/kg/min of ideal body weight, and monitor closely. Remodulin has not been studied in patients with severe hepatic insufficiency.
- Safety and effectiveness of Remodulin in pediatric patients have not been established.
- It is unknown if geriatric patients respond differently than younger patients. Caution should be used when selecting a dose for geriatric patients.
- There are no adequate and well-controlled studies with Remodulin in pregnant women. It is not known whether treprostinil is excreted in human milk or if it affects the breastfed infant or milk production.
Indication
Remodulin is a prostacyclin vasodilator indicated for the treatment of pulmonary arterial hypertension (PAH; WHO Group 1) to diminish symptoms associated with exercise. Studies establishing effectiveness included patients with NYHA Functional Class II-IV symptoms and etiologies of idiopathic or heritable PAH (58%), PAH associated with congenital systemic-to-pulmonary shunts (23%), or PAH associated with connective tissue diseases (19%).
In patients with PAH requiring transition from epoprostenol, Remodulin is indicated to diminish the rate of clinical deterioration. Consider the risks and benefits of each drug prior to transition.
REMISIhcpFEB2025
Please see accompanying Full Prescribing Information for Remodulin.
For additional information, visit www.RemodulinPro.com or call Customer Service at 1-844-UNITHER (1-844-864-8437).
References: 1. Remodulin [package insert]. Research Triangle Park, NC: United Therapeutics Corporation; 2023. 2. Tuder RM, Cool CD, Geraci MW, et al. Prostacyclin synthase expression is decreased in lungs from patients with severe pulmonary hypertension. Am J Respir Crit Care Med. 1999;159(6):1925-1932. 3. Lang IM, Gaine SP. Recent advances in targeting the prostacyclin pathway in pulmonary arterial hypertension. Eur Respir Rev. 2015;24(138):630-641. 4. Del Pozo R, Hernandez Gonzalez I, Escribano-Subias P. The prostacyclin pathway in pulmonary arterial hypertension: a clinical review. Expert Rev Respir Med. 2017;11(6):491-503.